"Uterine varicose veins" is a term many women hear in gynecology clinics, but few understand what it actually means. Far from being an isolated uterine problem, uterine varicosities are part of a broader venous disorder — pelvic venous insufficiency — that also explains a surprising amount of otherwise-unexplained chronic pelvic pain. In this article, Dr. Mohamed Haggag, consultant vascular surgeon in Heliopolis, Cairo, explains from a vascular surgery perspective what uterine varicose veins really are, how they differ from the more commonly discussed pelvic congestion syndrome, why they are missed for years, and how modern ovarian vein embolization resolves the symptoms without a hysterectomy.
What Are Uterine Varicose Veins?
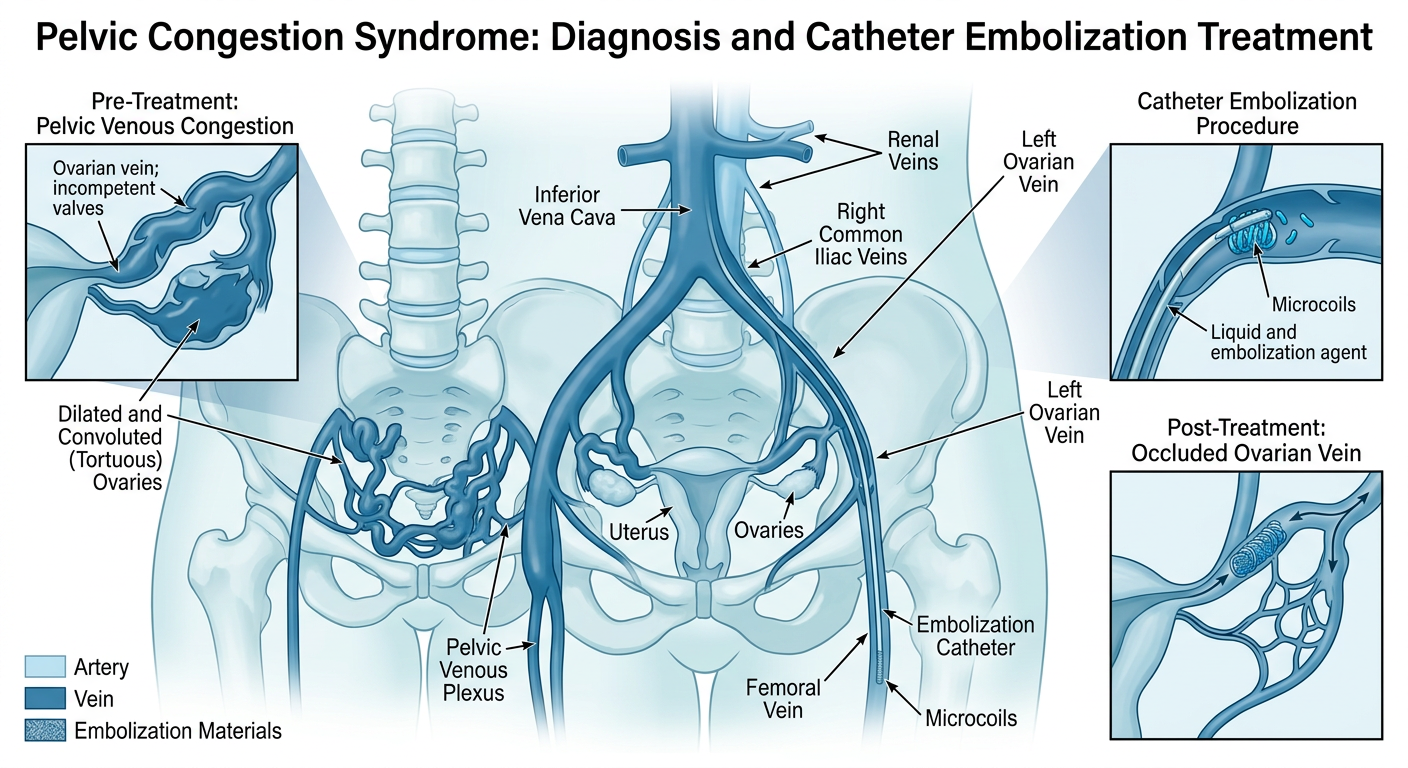
Uterine varicose veins (uterine varicosities) are dilated, tortuous veins of the uterine venous plexus — the network of veins surrounding the uterus. They develop when the ovarian veins or internal iliac veins lose their one-way valve function, allowing blood to reflux from the vena cava back down into the pelvis. Blood pools in the uterine, ovarian and pelvic plexuses, and those veins distend — exactly the same mechanism as varicose veins in the legs, but playing out deep inside the pelvis.
The key insight: uterine varicose veins are not a local uterine disease. They are the downstream expression of an anatomical problem with the ovarian and pelvic veins. That is why the correct treatment targets the ovarian veins — not the uterus itself.
Uterine Varicose Veins vs Pelvic Congestion Syndrome
The terms overlap significantly and are often used interchangeably, but there are useful distinctions:
- Pelvic Congestion Syndrome (PCS): The broader clinical umbrella — describes dilation of all pelvic venous plexuses (ovarian, uterine, vulvar, rectal). Uterine varicosities sit under this umbrella.
- Uterine varicose veins: A subset of PCS, referring specifically to the dilated peri-uterine plexus, often visible on transvaginal ultrasound as prominent serpiginous veins.
- Ovarian vein reflux: Usually the upstream cause — the incompetent valve in the ovarian vein drives the downstream pelvic and uterine varicosities.
- Vulvar varices: The external extension — varicosities visible in the vulva or inner thigh that are diagnostic of pelvic escape.
For a complete deep-dive on pelvic congestion syndrome, read Pelvic Congestion Syndrome: The Hidden Cause of Chronic Pelvic Pain.
Causes and Risk Factors
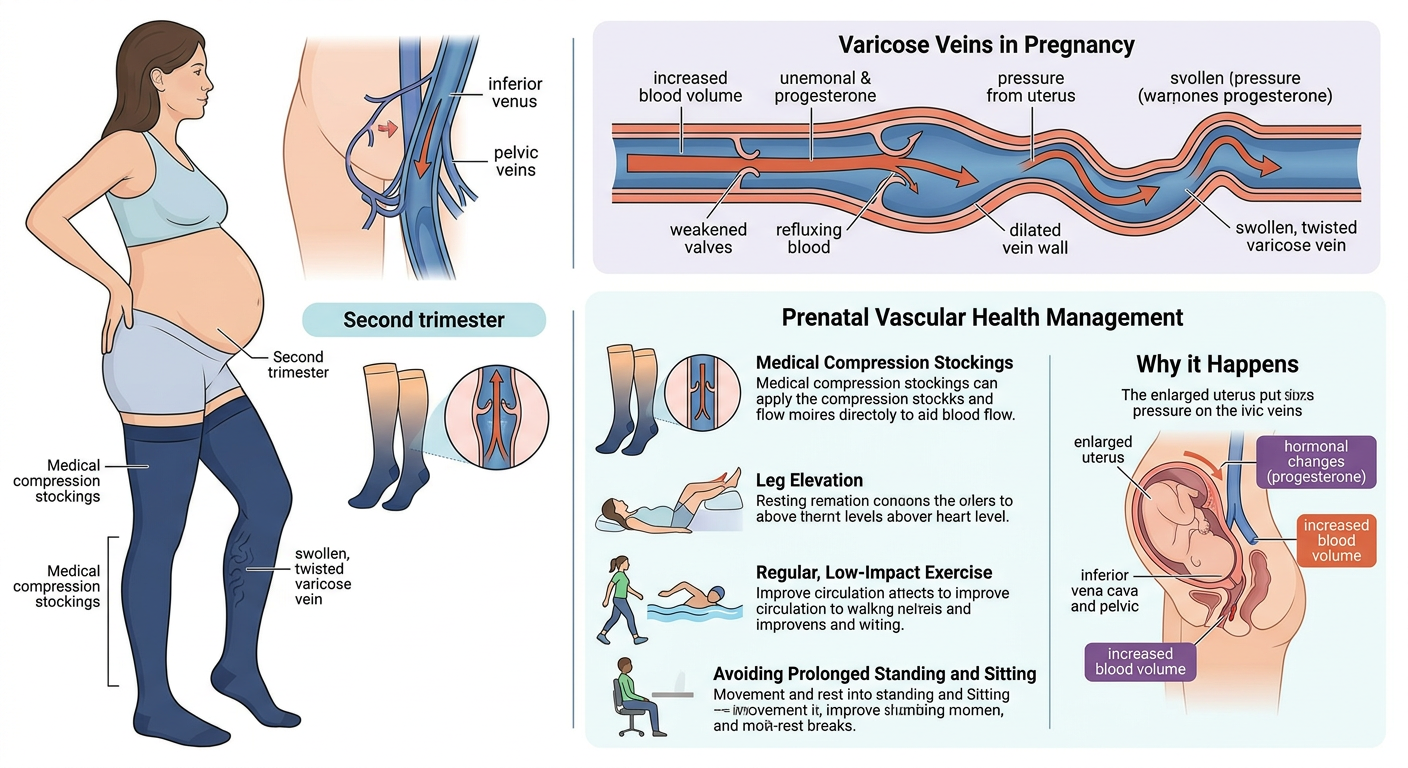
- Multiparity: Each pregnancy expands pelvic venous capacity. Three or more pregnancies is the single strongest risk factor.
- Hormonal factors: Estrogen relaxes the vein wall and predisposes to valvular reflux.
- Hereditary vein wall weakness: The same predisposition that causes leg varicose veins.
- Anatomical valveless ovarian vein: A congenital absence of valves — more common on the left.
- Nutcracker syndrome: Compression of the left renal vein between the aorta and SMA diverts blood into the left ovarian vein, driving reflux.
- Age: Most commonly diagnosed between 20 and 45 (reproductive years).
- Previous pelvic surgery: May injure pelvic veins and alter outflow.
Symptoms
Symptoms are often subtle and are frequently misattributed to chronic pelvic inflammatory disease or endometriosis:
- Chronic pelvic pain lasting 6 months or more — dull, heavy, aching — the cardinal symptom
- Pain worse at the end of the day, with prolonged standing, and relieved by lying down
- Dyspareunia (pain with intercourse) and post-coital ache — highly characteristic
- Irregular or heavy menstrual bleeding
- Cyclic flare — symptoms intensify before and during menses
- Visible varicosities in unusual locations: inner thigh, vulva, buttock
- Recurrent urinary symptoms — frequency, urgency, chronic dysuria without infection
- Generalized fatigue clustering with the pelvic symptoms
- Worsening after multiple deliveries
How Uterine Varicose Veins Are Diagnosed
- Transvaginal color Doppler: Visualizes dilated uterine and peri-uterine veins and documents reflux direction and velocity.
- Transabdominal pelvic ultrasound: A quick first-line screen.
- CT venography (CTV): Clearly shows dilated ovarian veins and rules out other causes such as Nutcracker syndrome.
- MR venography (MRV): Radiation-free alternative — preferred in women of reproductive age.
- Catheter venography: The gold standard — performed at the start of the embolization procedure itself; confirms the exact incompetent veins and allows immediate treatment.
Treatment Options
- Conservative measures: Analgesia, hormonal suppression, compression — may ease symptoms but do not address the anatomical cause.
- Ovarian vein embolization: The modern gold-standard treatment. Via a small groin or neck vein puncture, a microcatheter is guided into the incompetent ovarian veins and they are closed with fibered coils and/or a sclerosant. Day-case procedure, back to normal activity within 48 hours.
- Internal iliac vein embolization: Used when reflux involves the internal iliac system rather than (or in addition to) the ovarian veins.
- Sclerotherapy of vulvar varices: Direct injection for externally visible varices on the vulva or inner thigh.
- Hysterectomy: Not the rational treatment — the problem is venous, not uterine. It is reserved for cases that fail embolization or where there is another uterine condition independently requiring it.
Effect on Fertility and Pregnancy
A common and reasonable concern among patients of reproductive age is whether embolization affects fertility or future pregnancies. The answer is reassuring:
- Ovarian vein embolization does not impair fertility — the procedure targets the vein, not the ovary itself.
- Blocking the ovarian vein does not block the ovarian artery — ovarian blood supply and ovulation remain intact.
- Pregnancy after embolization is safe and successful in most patients.
- In fact, resolving pelvic congestion can improve conception in patients whose dyspareunia was preventing intercourse.
- A 3–6 month window is generally advised before attempting pregnancy after the procedure.
Chronic Pelvic Pain With No Clear Cause?
Book a specialist assessment at Dr. Mohamed Haggag's clinic in Heliopolis, Cairo, for accurate diagnosis of uterine and pelvic varicose veins with Doppler and venography — and, when indicated, minimally invasive ovarian vein embolization. Eleven years of dedicated vascular surgery experience.
Book a Consultation