Few medical emergencies are as immediately life-threatening as aortic dissection. When the inner lining of the aorta — the body's largest artery — tears, blood surges through the tear and splits the arterial wall into two layers, creating a false channel that can propagate rapidly in either direction. Without emergency treatment, the mortality risk rises by approximately 1–2% per hour. Dr. Mohamed Haggag, vascular surgeon in Heliopolis, Cairo, explains how to recognise this emergency and what modern treatment involves.
Dissection vs. Aneurysm: A Critical Distinction
The two conditions are often confused, but they are fundamentally different:
- Aortic aneurysm: All three layers of the aortic wall weaken and bulge outward together. It is a slow, often silent process — typically managed electively when the aneurysm reaches a threshold size.
- Aortic dissection: The inner layer (intima) tears, and blood forces its way between the intima and the outer layers (media and adventitia), creating a false lumen. This is almost always acute and is a surgical emergency.
Although the names sound similar in Arabic ("تمدد الأبهر" vs "تشريح الأبهر"), they represent entirely different pathologies with different urgency levels and treatments.
How Does Dissection Happen?
The tear typically originates in the ascending aorta (just above the heart) or just beyond the left subclavian artery in the descending aorta. Once the intima tears, pulsatile arterial pressure drives blood into the wall with each heartbeat, propagating the dissection — sometimes the entire length of the aorta — within seconds to minutes.
The false lumen can compress branch arteries along its path, causing malperfusion to the heart (coronary arteries), brain (carotid arteries), kidneys, spine, or limbs — each generating its own constellation of symptoms.
Stanford Classification: Type A and Type B
The Stanford system is the most widely used classification, based on whether the ascending aorta is involved:
- Stanford Type A: Involves the ascending aorta (regardless of where the tear originates). Accounts for ~65% of cases. Mortality without surgery is 50% within 48 hours. Requires emergency open cardiac surgery.
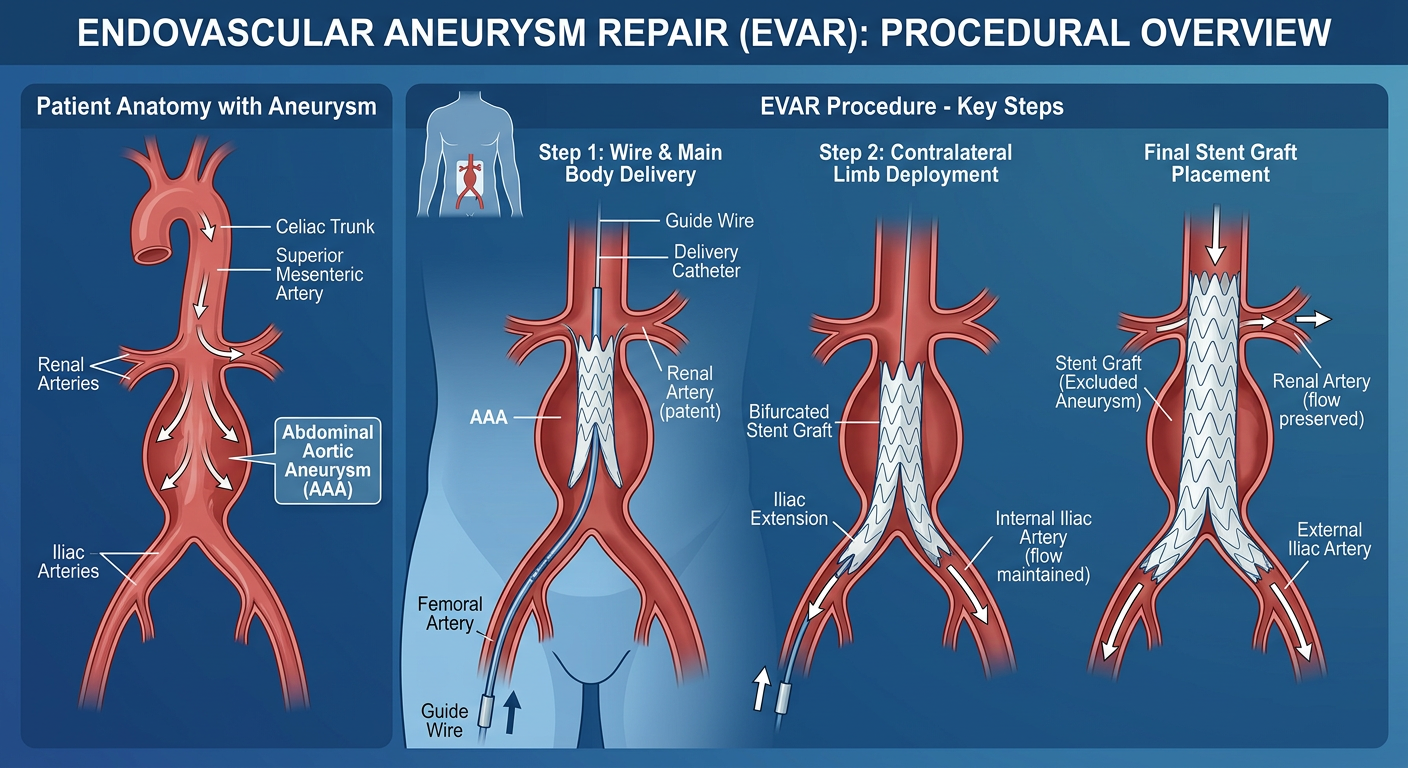
- Stanford Type B: Confined to the descending aorta (beyond the left subclavian artery). Often managed initially with intensive medical therapy (strict blood pressure control). Complicated Type B dissections — with malperfusion, rupture, or rapid expansion — are treated with TEVAR (Thoracic Endovascular Aortic Repair), a minimally invasive stent-graft procedure.
Risk Factors
The leading risk factors for aortic dissection are:
- Severe, uncontrolled hypertension — the most important modifiable risk factor, present in 70–80% of patients
- Marfan syndrome and other connective tissue disorders (Loeys-Dietz, Ehlers-Danlos)
- Bicuspid aortic valve — congenital abnormality that predisposes the aorta to dilation and tear
- Coarctation of the aorta
- Cocaine use — causes acute hypertensive surges
- Pregnancy — third trimester and peripartum period carry elevated risk, especially in women with connective tissue disorders
- Prior aortic surgery or instrumentation
Diagnosis: Emergency CT Angiography
When aortic dissection is suspected, the investigation of choice is contrast-enhanced CT angiography (CTA) of the chest, abdomen, and pelvis. It is fast (completed in minutes), highly accurate (sensitivity and specificity > 98%), and shows the full extent of the dissection, the true and false lumens, and any branch vessel involvement.
Transoesophageal echocardiography (TOE) is an alternative when CTA is not immediately available or when the patient is too unstable to be moved. MRI, while highly accurate, is too slow for acute management.
Treatment by Type
Type A: Emergency Surgery
Type A dissection is treated with emergency open surgery performed by a cardiac surgeon. The goals are to:
- Replace the ascending aorta with a synthetic graft
- Close the intimal tear to eliminate blood flow into the false lumen
- Repair or replace the aortic root and valve if involved
- Restore blood flow to coronary and carotid arteries if compromised
Operative mortality ranges from 15–25% in major aortic centres, but the alternative — no surgery — carries near-certain early death.
Type B: Medical Therapy and TEVAR
Uncomplicated Type B dissections are managed with aggressive medical therapy: intravenous beta-blockers and vasodilators to keep systolic blood pressure below 120 mmHg and heart rate below 60 bpm. This reduces the haemodynamic stress on the aortic wall and allows the false lumen to thrombose.
Complicated Type B dissections (those with malperfusion, rapid expansion, or imminent rupture) are treated with TEVAR — a catheter-delivered stent-graft deployed over the intimal tear to seal it and redirect blood into the true lumen. This endovascular approach has largely replaced open surgery for Type B in expert centres.
Long-Term Follow-Up
Survivors of aortic dissection require lifelong surveillance. The false lumen may persist, gradually dilate, and — years after the acute event — require further intervention. Follow-up CT or MRI of the entire aorta is typically performed at 1, 3, 6, and 12 months, then annually. Blood pressure targets are stricter than for the general population.
Aortic Disease Concerns? Get Expert Assessment
If you have risk factors for aortic disease — uncontrolled hypertension, Marfan syndrome, bicuspid aortic valve, or a family history of aortic emergency — Dr. Mohamed Haggag can arrange appropriate screening and follow-up.
Book a Consultation